Post-ACLR Recovery: Linking strength, jump and patient outcomes
Study Information
Dutaillis, B., Collings, T., Bellinger, P., Timmins, R. G., Williams, M. D., & Bourne, M. N. (2025). Time‐course changes in lower limb strength, vertical jump metrics and their relationship with patient reported outcomes following anterior cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy, 1–16.
https://doi.org/10.1002/ksa.12694
Purpose of the Study
Field-based measures of lower-limb strength and vertical jump performance are increasingly used in clinical practice among young athletes recovering from anterior cruciate ligament reconstruction (ACLR). No studies have examined how such measures change across the time course of rehabilitation, and little is known about the relationship between objective measures of lower-limb function and patient-reported outcome measures (PROMs).
This study aimed to provide greater insight into how field-based measures of objective lower-limb function change throughout recovery and their relationship with anterior cruciate ligament return to sport index (ACL-RSI) and knee injury osteoarthritis outcome scores (KOOS).
Methods
Thirty recreationally active athletes (11 females, 19 males; aged 16-34 years) were invited to complete a field-based testing battery at four regular time points (3, 6, 9 and 12 months) throughout their first year of recovery following primary ACLR.
The testing battery included assessments using ForceDecks, DynaMo, NordBord and ForceFrame, as well as PROMs, and consisted of:
Objective assessments
- Countermovement jump (CMJ)
- Single leg jump (SLJ)
- Drop jump (DJ)
- Single leg drop jump (SLDJ)
- Isometric knee extension strength
- Eccentric knee flexion strength (Nordic curl)
- Isometric hip abduction and adduction strength
PROMs
- ACL-RSI
- KOOS
Linear and non-linear mixed models, with a time-by-limb interaction, were used to explore how all measures changed from 3 to 12 months in both the reconstructed and uninjured contralateral limbs. In simple terms, these analyses allowed the researchers to track recovery patterns over time in both limbs and to test whether the reconstructed limb improved differently compared with the uninjured limb.
To determine which objective measures of lower-limb function most effectively distinguished between individuals with higher and lower levels of psychological readiness and perceived recovery following ACLR, mixed-model decision trees were used.
Key Findings
- Faster Recovery: Most measures (~71%) of lower-limb strength and vertical jump performance displayed a faster rate of recovery in the reconstructed limb from 3 to 6 months, followed by a continued but slower rate up to 12 months following ACLR.
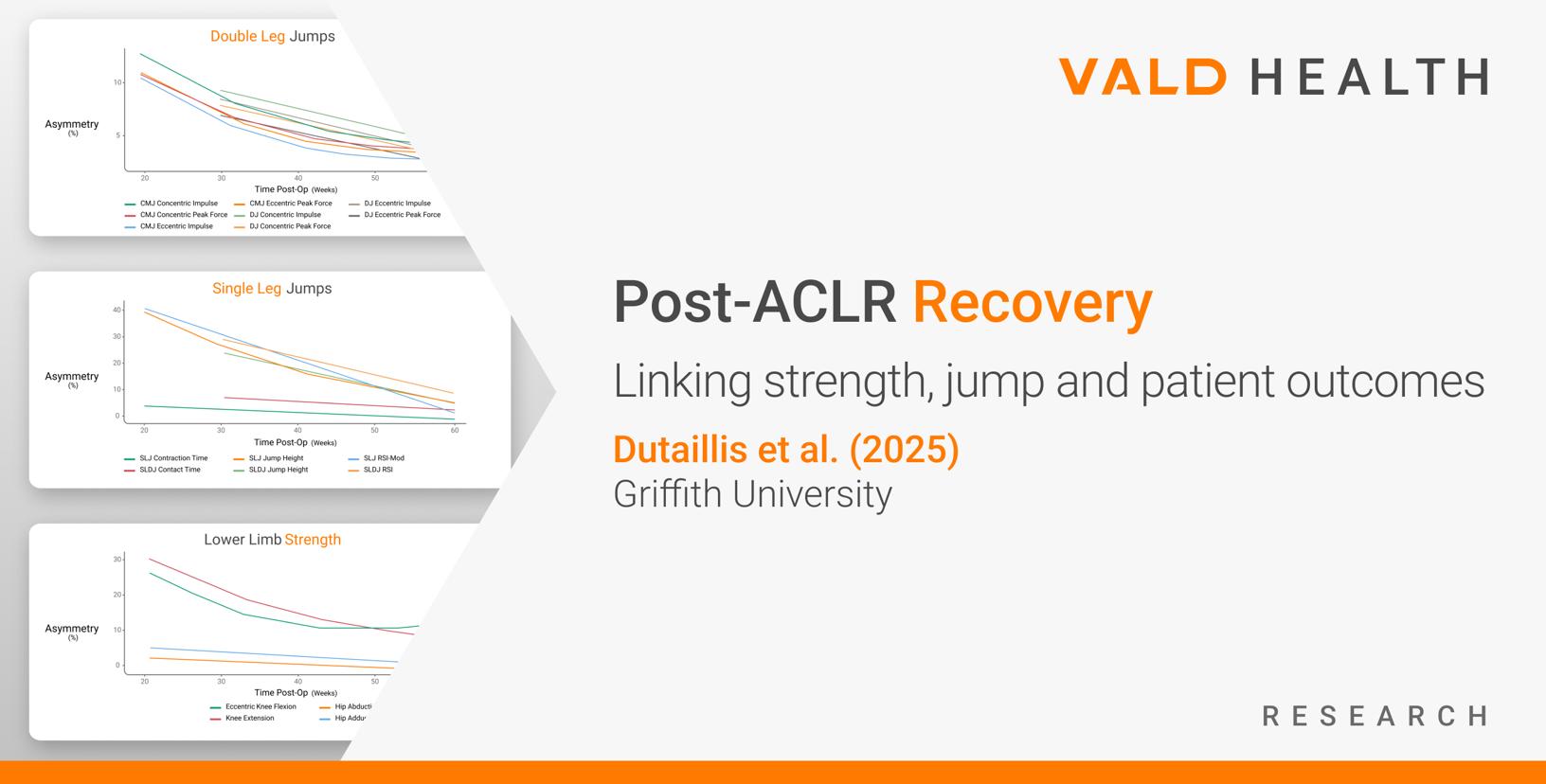
- Reduced Asymmetry: Most metrics (~70%) showed significant between-limb asymmetry reduction, with most reaching <10% asymmetry by the 12-month time point.
- Jump Height Linked to Readiness: SLJ jump height for the ACLR limb explained 67% of variance in ACL-RSI score (r² = 0.67), with a cut-off value of 8.4cm best discriminating between higher and lower scores (35 vs. 72).
- Strength Asymmetry Related to Self-Reported Function: Knee extension peak force asymmetry explained the most variation in KOOS scores (r² = −0.78), with a cut-off value of 38.3% best discriminating between higher and lower scores (65 vs. 82).
…lower-limb strength and vertical jump performance displayed a faster rate of recovery in the reconstructed limb from 3 to 6 months…[and] showed significant between-limb asymmetry reduction [by 12 months]…
Time-course changes in jump height, contact or contraction time and reactive strength index (RSI) for CMJ, SLJ, DVJ and SLDJ. Significant effects (p < 0.05) of the mixed models are indicated in the top right of each plot (T = time, L = limb and X = time × limb).
Time-course changes in lower-limb strength measures. Significant effects (p < 0.05) of the mixed models are indicated in the top right of each plot (time = T, limb = L and time × limb = X).
Time-course changes in between-limb asymmetry for double leg (left) and single leg (right) CMJ and DJ metrics, along with lower-limb strength (bottom) measures.
Mixed-model decision trees for ACL-RSI and KOOS. Terminal nodes (blue) display the number of observations and the mean score with 95% confidence intervals (CIs). Red numbers indicate the between-node effect size (Cohen’s d).
Practical Applications
For practitioners working with young athletes following primary ACLR, the following results show the average recovery rate of the ACLR limb that can be expected over a 3-month period.
| VALD System | Test | Metric | Mean Change per 3 Months in ACLR Limb (95% CI) |
| ForceDecks | CMJ | Concentric peak force | 52.0N [35.6, 68.3] |
| Concentric impulse | 9.3N.s [5.5, 13.0] | ||
| Eccentric peak force | 73.2N [54.4, 92.0] | ||
| Eccentric impulse | 4.4N.s [1.4, 7.4] | ||
| SLJ | Jump height | 2.3cm [1.7, 2.8] | |
| Contraction time | -0.01s [-0.03, 0.01] | ||
| RSI-modified | 0.03 [0.02, 0.04] | ||
| DJ | Concentric peak force | 80.2N [31.8, 128.6] | |
| Concentric impulse | 5.3N.s [-1.3, 11.8] | ||
| Eccentric peak force | 63.8N [-72.1, 199.7] | ||
| Eccentric impulse | -0.2N.s [-9.3, 8.9] | ||
| SLDJ | Jump height | 1.9cm [1.1, 2.6] | |
| Contact time | -0.05s [-0.08, -0.02] | ||
| RSI | 0.06 [0.04, 0.08] | ||
| DynaMo | Isometric knee extension 90° | Peak force | 67.5N [48.0, 87.1] |
| NordBord | Nordic hamstring curl test | Peak force | 31.5N [18.1, 44.9] |
| ForceFrame | Isometric hip abduction | Peak force | 6.2N [2.13, 10.3] |
| Isometric hip adduction | Peak force | 6.5N [1.0, 11.9] |
Knee extension and flexion peak force, and most vertical jump metrics in the uninjured contralateral limb, changed across rehabilitation. Practitioners should be mindful that this will impact changes in limb symmetry indices and potentially cause an overestimate or underestimate of recovery of the reconstructed limb.
Normative values for lower-limb strength and vertical jump performance of age-, sex- and sport-matched populations may provide practitioners with additional targets for return-to-play (RTP) criteria.
RSI is commonly used as a performance criterion in team sports and has been proposed as a key RTP criterion following ACLR. However, the results show that changes in RSI, in all jump types, are mostly driven by increasing jump height.
…results show that changes in RSI, in all jump types, are mostly driven by increasing jump height.
Contact and contraction times changed very little over time and displayed little to no between-limb differences in SLJs. As such, it is unclear if further information is gained by tracking RSI vs. jump height alone.
Finally, strong relationships were observed between SLJ jump height, knee extension strength, and the ACL-RSI and KOOS PROMs across rehabilitation. While these findings do not establish cause and effect, they suggest that poor SLJ height may indicate limited psychological readiness to return to sport (RTS), and that large knee extension peak force asymmetry may be associated with greater perceived knee pain and disability during rehabilitation.
…poor SLJ height may indicate limited psychological readiness to RTS, and large knee extension peak force asymmetry may be associated with greater perceived knee pain and disability…
However, practitioners should be mindful that there may be some cyclic interplay between these. Improved strength and dynamic function may lead to greater athlete confidence and fewer adverse symptoms. Alternatively, a reduction in pain and fear of reinjury may allow an athlete to move more freely with improved force and performance output.
If you would like to learn how VALD’s measurement technology can support ACL rehabilitation, track recovery and guide return-to-play decisions, download our Practitioner’s Guide to ACL or get in touch with our team.