Understanding the Drop Jump
What Is a Drop Jump?
The drop jump (DJ) is an assessment used in sports performance and rehabilitation to evaluate reactive strength and stretch-shortening cycle (SSC) function. It involves dropping off a raised platform (commonly a box), landing on both feet and immediately jumping vertically with maximal effort and minimal ground contact time (GCT).
This assessment primarily evaluates fast SSC (defined by GCTs <250ms) mechanics and reactive strength capabilities. Fast SSC characteristics are defined by GCTs less than 250ms; however, lack of experience with these tests often leads even high-performing patients to have GCTs above this threshold.
A patient performing a DJ with a step-out strategy (one limb leads off the box). Note: Asymmetry values may change depending on DJ strategy.
The SSC is a neuromuscular process in which a rapid eccentric contraction stores elastic energy (in the form of tensile strain) in the muscle’s tendons (Komi, 2000). This energy is then quickly returned during the concentric phase, amplifying the total force produced.
Fast SSC mechanics underpin a patient’s reactive strength abilities, where SSC characteristics combine with proper neuromuscular sequencing to create the building blocks of reactive strength development. Reactive strength is commonly used as a proxy to gauge a patient’s neuromuscular capabilities that support movements in activities requiring quick force generation like sprinting, change of direction and plyometric movements in sport.
…SSC characteristics…create the building blocks of reactive strength development.
During a well-executed DJ, GCTs are extremely brief, ideally less than 250ms (Ünver et al., 2024). This short transition time is crucial for utilizing stored elastic energy to maximize jump height. As long as overall performance (e.g., jump height) is maintained or improved, a faster GCT indicates a more reactive patient.
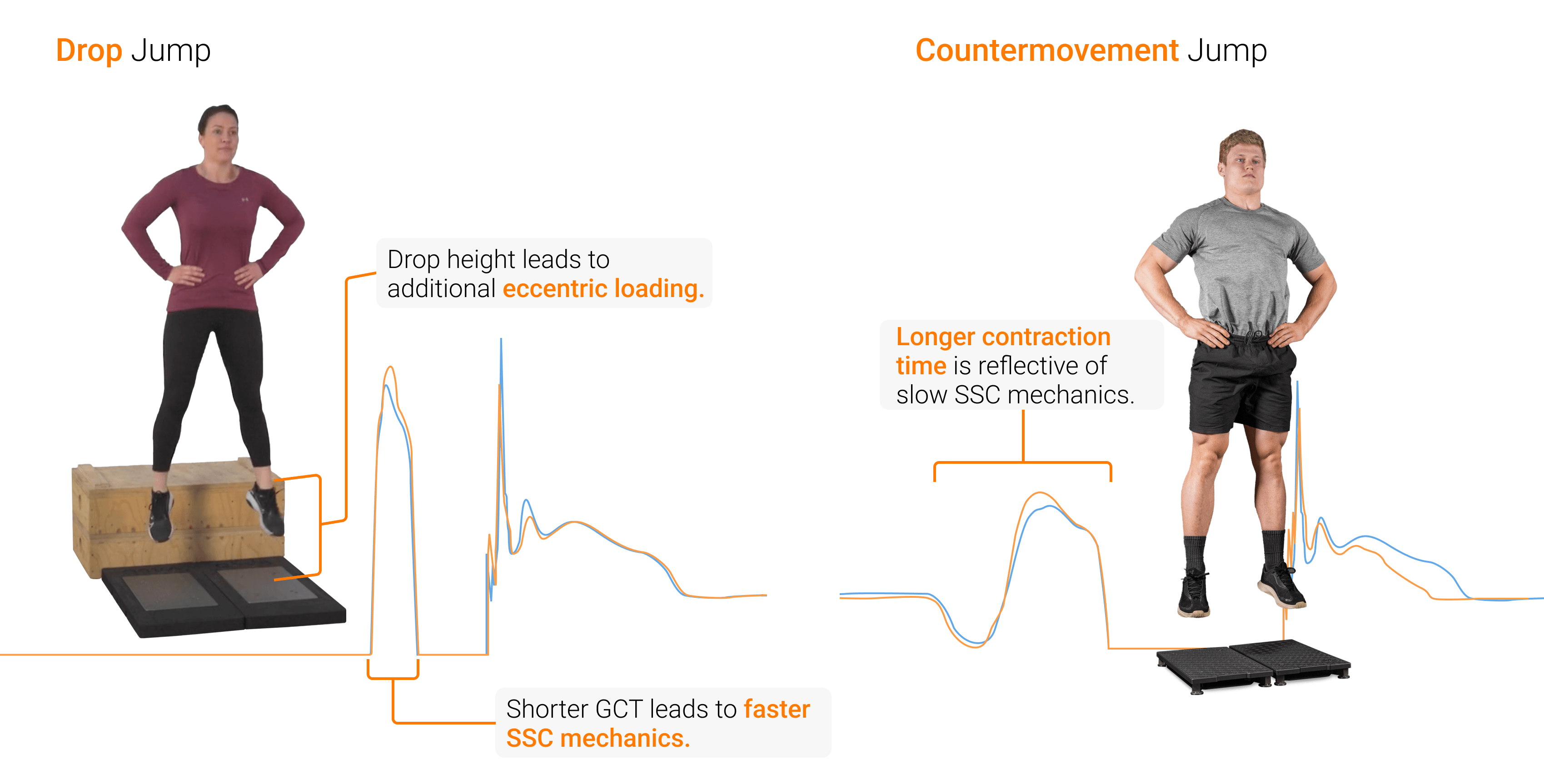
Unlike the countermovement jump (CMJ), which starts from a standing position, the DJ adds greater eccentric demand through a controlled free fall from a predetermined height. This test is ideal for practitioners looking to assess a patient’s ability to cope with impact forces for elite jump performance. However, practitioners looking to assess slow SSC mechanics (>250ms contraction time) may be better suited to use the CMJ.
Many of sports’ most mechanically damaging loads come from high-impact landings and deceleration, as opposed to actions that bias concentric forces (Harper et al., 2024). Therefore, testing – and preparing – patients for the forces they will actually encounter in sport and activity is essential.
…sports’ greatest loads come from high-impact landings and deceleration… Therefore, [testing the forces] they will actually encounter in sport and activity is essential.
Benefits of the DJ Assessment
Practitioners who understand the mechanics and applications of the DJ can significantly enhance assessment insights and, in turn, improve their training methodologies across multiple domains.
The DJ is a relevant performance proxy measurement and a helpful diagnostic tool that can provide meaningful insights to guide training decisions.
The DJ is a relevant performance proxy measurement and a helpful diagnostic tool that can provide meaningful insights to guide training decisions.
Health and performance practitioners can assess various components of lower extremity function, including impact and deceleration characteristics, force production capabilities and movement strategy during high-intensity plyometric assessments like the DJ.
Integrating force plate technology can capture detailed metrics that highlight those characteristics, including GCT, flight time, reactive strength index (RSI) and over 100 other performance and health metrics.
For a full list of metrics and definitions, refer to the ForceDecks Technical Glossary.
Integrating assessments with multiple performance technologies, such as force plates and visual aids (e.g., ForceDecks Vision), enables practitioners to link movement changes to force-related impairments. These objective measurements provide progress tracking and training insights, offering greater certainty that patients are on the right path.
The protocol for performing a standardized DJ is outlined below, highlighting each phase and common faults.
| Phase | Description | Common Faults |
|---|---|---|
| 1. Drop Phase | The patient stands on a raised platform and steps off, maintaining vertical alignment during the drop while preparing for ground contact |
|
| 2. Eccentric | The patient decelerates their momentum through small amounts of triple flexion (simultaneous flexion through the hip, knee and ankle), maintaining a stiff upper and lower body |
|
| 3. Amortization [Moment of 0 Velocity] | The patient continues to exert high forces in a brief isometric phase as they transition and redirect their downward momentum upwards |
|
| 4. Concentric | The patient accelerates their momentum upwards to jump as high as possible |
|
| 5. Flight | The period during which the patient is airborne from the previous jump |
|
| 6. Jump Landing | The patient decelerates their downward momentum after contacting the force plates, maintaining even support and a balanced posture |
|
Metric Selection for the DJ
For practitioners first assessing the DJ, simple metrics like jump height, GCT, RSI and peak landing force asymmetry help to provide a well-rounded perspective of a patient’s performance.
…jump height, GCT, RSI and peak landing force asymmetry help to provide a well-rounded perspective of a patient’s performance.
| Metric | Definition | Insights |
|---|---|---|
| Jump Height | Maximum vertical displacement of the CoM between takeoff and landing | Jumping performance and overall plyometric capacity |
| GCT | Time period between drop landing and takeoff | SSC efficiency and utilization |
| RSI | The ratio of jump height (measured via the impulse-momentum calculation or flight time calculation) to contact time | Reactive strength capacity |
| Peak Drop Landing Force Asymmetry | Percent difference in force production between right and left limbs at maximum vertical force during the landing phase | Jumping strategy and lower limb dominance during plyometric activities |
Visualizing all of these metrics at once helps practitioners make sense of the key performance attributes their patients need to train for optimal performance, simplifying the training periodization process.

VALD Hub’s configurable patient profiles can display and track multiple DJ metrics over time.
Practitioners may select different drop heights based on the patient’s training status and the specific qualities being assessed. Lower drop heights (20-30cm) are often used for patients with lower plyometric experience or rehabilitation settings, while patients with greater DJ experience may benefit from higher drops (40-60cm) to maximize reactive strength development (Sanders et al., 2024). However, excessively high drops can compromise technique and increase injury risk without additional performance benefits.
For more information on determining proper height for DJ assessments and training, check out the DJ height profile on page 50 of the Practitioner’s Intermediate Guide to Force Plates.
As noted previously, a common fault occurs when a patient lowers their CoM before stepping off the box, effectively lowering the height that their CoM drops from. ForceDecks uses reverse integration calculations from the landing phases to calculate the patient’s effective drop height (EDH). This calculation not only ensures the accuracy of the data collected but also provides technical feedback to the practitioner and patient, determining if the EDH and box height are significantly different.
[ForceDecks calculates]…the patient’s EDH …[to ensure] the accuracy of the data collected…
Key Physical Traits Required for the DJ
Although the DJ is an effective, efficient and relatively scalable assessment, even its most regressed options (e.g., performing a DJ with a drop height of 10cm) still pose a significant plyometric load to the patients. Therefore, it is important to assess and ensure that patients have adequate exposure and capacity in the following performance qualities:
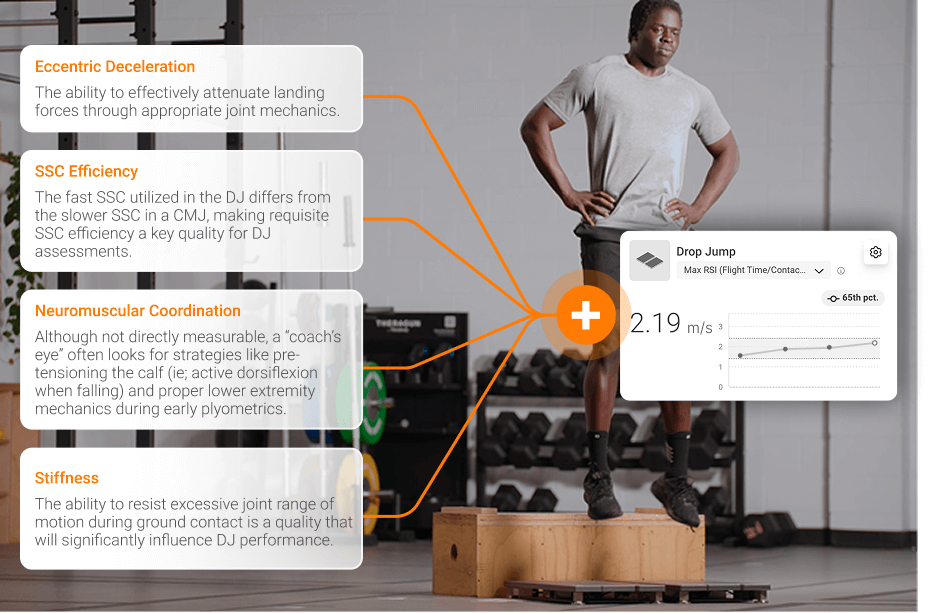
Four performance qualities related to DJ performance.
Common Applications of the DJ Assessment
Once a patient is ready to perform a DJ, practitioners have a wide range of options to integrate and apply the assessment (and its results) to their practice.
…practitioners have a wide range of options to integrate and apply the assessment (and its results) to their practice.
High-performance personnel, including strength and conditioning coaches, often use DJ assessments for a few key insights (Kipp et al., 2018), such as:
- Assessing plyometric ability and reactive strength.
- Monitoring adaptations to physical performance and sport training.
- Identifying movement strategy during high-velocity movements.
- Evaluating landing mechanics and potential injury risk factors that may not show up in slower, less eccentrically demanding movements.
Similarly, end-stages of rehabilitation may include DJ assessments to best determine which rehabilitation qualities a patient still needs to develop (Pedley et al., 2025). Some of these insights include:
- Assessing readiness (e.g., tissue tolerance and capacity) for higher impact activities as patients progress through rehabilitation.
- Evaluating landing control and rapid deceleration capabilities.
- Performing return-to-sport testing for lower limb injuries.
- Continued monitoring of physical qualities after return to sport has occurred.
However, practitioners should exercise caution when interpreting improvements in DJ performance in rehabilitation settings. Improvements often occur due to a technical optimization of the task, rather than true neuromuscular improvements.
DJ results analysis enables practitioners to design tailored training programs based on patients’ unique strengths and weaknesses. These programs are often implemented to enhance reactive strength and fast SSC function, crucial components for sports requiring explosive acceleration, deceleration and plyometric loads.
DJ results analysis enables practitioners to design tailored training programs based on patients’ unique strengths and weaknesses.
Similarly, the DJ provides reliable, objective data on a patient’s ability to tolerate high eccentric loads and rapid force production – essential criteria for a safe return to high-intensity sporting activities (Markwick et al., 2015).
Rebound Jump Assessments: Which should you choose?
The DJ, hop test (HT) and countermovement rebound jump (CMRJ) each assess reactive neuromuscular qualities, creating different demands and associated movement strategies of patients. All three jumps are considered rebound jumps, where a patient lands (either from a box or from a previous jump) and immediately jumps again with minimal GCT. However, each jump has a unique characteristic, serving its own purpose:
- DJ: The DJ is considered to be the most advanced of the three rebound jump assessments because it can be made more challenging by increasing the drop height. This allows for maximal effort profiling and monitoring of long-term training adaptations over time.
- HT: Typically performed in clusters of 5 to 10 reps, the HT assesses a patient’s ability to repeatedly produce force and withstand impact under rhythmic, elastic conditions. It emphasizes consistency across multiple efforts, offering insights into average performance and fatigue resistance during rebound jumping. Because each jump starts and ends at the patient’s self-selected height, it provides a continuous, cyclical stimulus without the psychological barrier of an external drop.
- CMRJ: The CMRJ involves a single maximal effort followed immediately by one reactive rebound. Designed to mimic the stretch-shortening cycle demands of a DJ, the CMRJ focuses on quality over quantity – capturing key metrics like contact time, jump height and RSI from just one effort. Its self-limiting nature, where the drop height is determined by the initial CMJ, makes it particularly useful for evaluating high-intensity reactivity in more sensitive or early-stage populations.
Rebound jumps [involve] a patient landing (either from a box or from a previous jump) and immediately jumps again with minimal GCT.
Each assessment provides unique value when used at the right time. Practitioners should consider both what the test measures and how demanding it feels for the patient. In many cases, the patient’s ability to complete the test comfortably will matter more than the specific performance quality being assessed.
Conclusion
The DJ stands as a powerful assessment tool that bridges the gap between laboratory testing and real-world sporting demands. Its ability to evaluate reactive strength and fast SSC function makes it invaluable for both performance enhancement and rehabilitation contexts.
With systems like ForceDecks, the DJ test can be automatically detected and analyzed with minimal manual input, streamlining the testing process and ensuring consistency. ForceDecks provides over 100 metrics from a single test, allowing practitioners to measure and monitor key qualities like jump height, contact time, RSI and phase-specific forces, giving practitioners a comprehensive view of a patient’s performance and movement strategy.
This level of detail allows for more accurate identification of the physical qualities that need to be developed to improve performance or reduce injury risk. Whether guiding a patient through rehabilitation or pushing the boundaries of their potential, the technology-enabled DJ test offers a clear window into the dynamic and complex nature of human movement under high-intensity conditions.
If you would like to know more about the DJ or the value of implementing technology into your organization, please reach out.
References
- Komi, P. V. (2000). Stretch-shortening cycle: a powerful model to study normal and fatigued muscle. Journal of Biomechanics, 33(10), 1197–1206. https://doi.org/10.1016/s0021-9290(00)00064-6
- Ünver, E., Konşuk Ünlü, H., Yıldız, A. E., & Cinemre, Ş. A. (2024). A new approach for classification of stretch-shortening cycle: Beyond 250 ms of ground contact time. Journal of Sports Sciences, 42(17), 1617–1626. https://doi.org/10.1080/02640414.2024.240387
- Harper, D., Cervantes, C., Van Dyke, M., Evans, M., McBurnie, A., Dos' Santos, T., Eriksrud, O., Cohen, D. D., Rhodes, D., Carling, C., & Kiely, J. (2024). The braking performance framework: Practical recommendations and guidelines to enhance horizontal deceleration ability in multi-directional sports. International Journal of Strength and Conditioning, 4(1). http://dx.doi.org/10.47206/ijsc.v4i1.351
- Sanders, G. J., Skodinski, S., & Peacock, C. A. (2024). Analyzing the impact of various jump load intensities on countermovement jump metrics: A comparison of average, peak, and peak-to-average ratios in force-based metrics. Sensors, 25(1), 151–151. https://doi.org/10.3390/s25010151
- Kipp, K., Kiely, M. T., Giordanelli, M. D., Malloy, P. J., & Geiser, C. F. (2018). Biomechanical determinants of the reactive strength index during drop jumps. International Journal of Sports Physiology and Performance, 13(1), 44–49. https://doi.org/10.1123/ijspp.2017-0021
- Pedley, J. S., Lloyd, R. S., Read, P. J., Moore, I. S., Myer, G. D., & Oliver, J. L. (2025). Drop jump vertical kinetics identify male youth soccer players at greater risk of non-contact knee injury. Physical therapy in sport: Official Journal of the Association of Chartered Physiotherapists in Sports Medicine, 73, 48–56. Advance online publication. https://doi.org/10.1016/j.ptsp.2025.03.003
- Markwick, W. J., Bird, S. P., Tufano, J. J., Seitz, L. B., & Haff, G. G. (2015). The intraday reliability of the reactive strength index calculated from a drop jump in professional men's basketball. International Journal of Sports Physiology and Performance, 10(4), 482–488. https://doi.org/10.1123/ijspp.2014-0265