Return to work with HumanTrak (Use Case)
Available in:
EN
Using HumanTrak to improve the recovery pathway following a rotator cuff tear workplace injury.
Problem
Bruce, a 57-year-old miner, was working the second of his three rostered weeks. He was lifting mining equipment to a high shelf, a task he completes many times per day, when he experienced a sharp pain in his right shoulder and could no longer lift any weight. Bruce sought medical attention immediately and was deemed unfit to work. Bruce returned home and visited his General Practitioner (GP) who diagnosed his injury as rotator cuff tear with associated shoulder bursitis caused by overuse and granted him a work cover claim, which included five free physiotherapy sessions. Bruce was instructed to rest his shoulder and visit his local physiotherapist for treatment.
Rehabilitation: phase 1
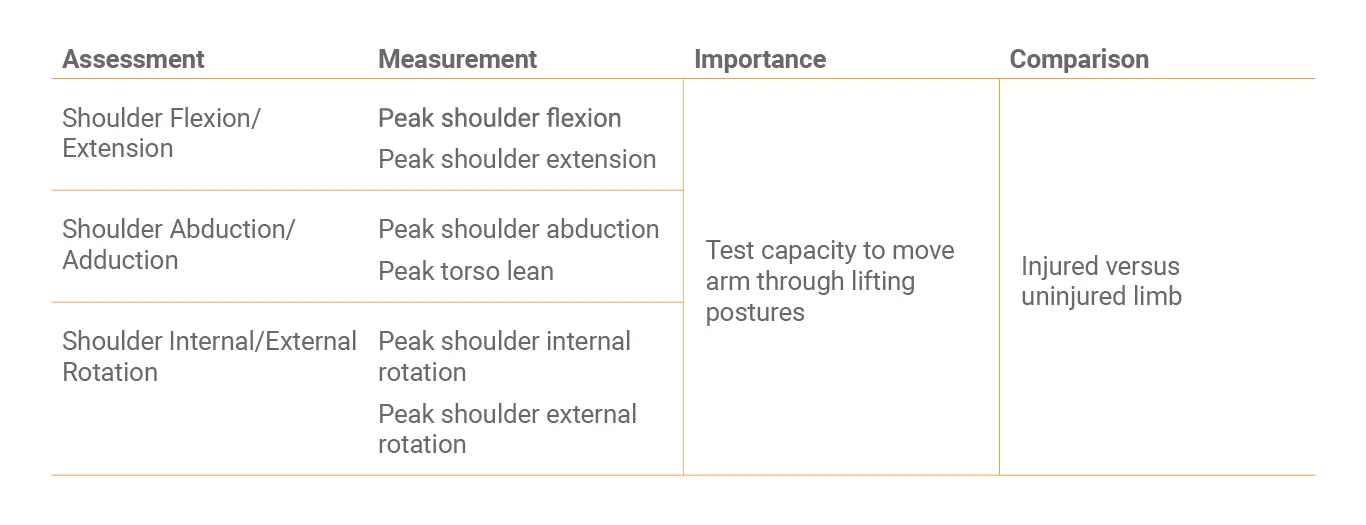
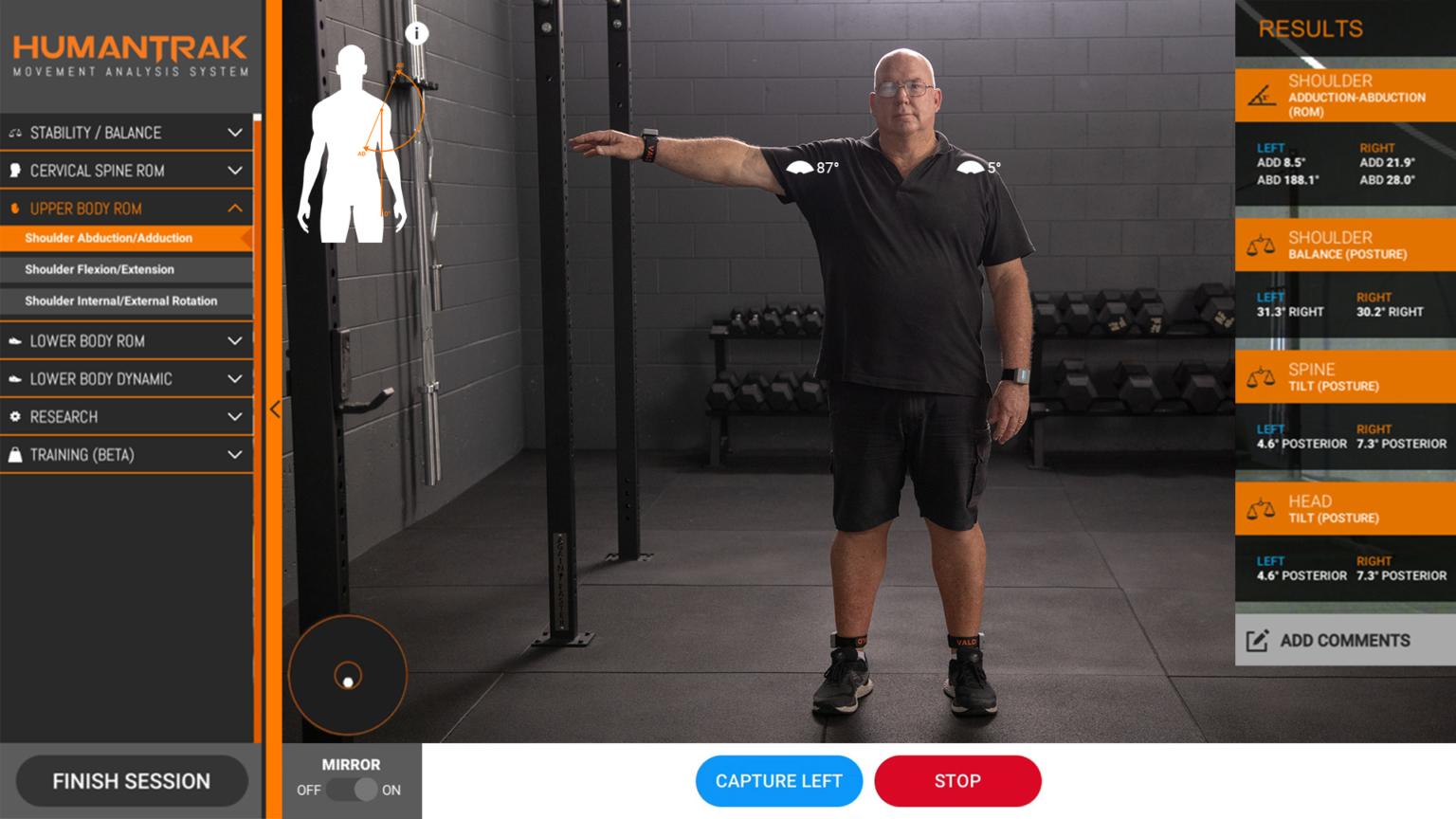
Bruce attended his local physiotherapist for an initial consultation. The physiotherapist reviewed Bruce’s medical certificate and proceeded with initial subjective and objective assessments. The physiotherapist determined the mechanism of injury as acute episode induced by lifting equipment overhead at work, reviewed the history of pain, and confirmed Bruce’s rehabilitation goals. Bruce’s physiotherapist recorded Bruce’s perceived level of pain when performing shoulder abduction, flexion, and external rotation, and when palpating the top of the shoulder. The limited shoulder range of motion and tenderness of the shoulder area confirmed the shoulder bursitis diagnosis from the GP. To capture baseline range of motion and determine the magnitude of asymmetry between arms, Bruce completed shoulder flexion/extension, abduction/ adduction, and internal/external rotation HumanTrak assessments. Bruce presented initially with frozen shoulder that prevented pain-free movement of the shoulder to an abducted position. Therefore, shoulder internal/external rotation was performed with no shoulder abduction.
Bruce immediately reviewed the on-screen test results with his physiotherapist and could clearly see the difference in shoulder abduction range of motion on his injured shoulder compared to his healthy shoulder. The physiotherapist also captured baseline shoulder strength using VALD’s portable ForceFrame strength testing system, which clearly showed reduced strength on Bruce’s injured side. To address the ROM discrepancy, the physiotherapist prescribed daily stretching exercises and instructed Bruce to continue taking anti-inflammatories and applying ice to the area. A follow-up appointment was scheduled one week later. After the session, the physiotherapist quickly emailed the HumanTrak report to Bruce and attached it to Bruce’s Patient Management Software profile.
Rehabilitation: phase 2
Bruce returned for four subsequent sessions, in which progression from the initial assessment was measured using pain scales, shoulder abduction ROM and torso lean from HumanTrak, and isometric strength using the ForceFrame. In subsequent sessions, the HumanTrak report revealed to Bruce how he was excessively leaning his torso to one side to compensate for the limited shoulder abduction range of motion (ROM) . The physiotherapist advised Bruce that the torso lean may put excessive strain on his spine and place him at risk of sustaining a back injury.
Once pain had reduced, the physiotherapist prescribed exercises to strengthen the surrounding shoulder muscles to ease pain and reduce the likelihood of recurrence. Following each session, the physiotherapist was able to maintain Bruce’s engagement in treatment by clearly showing shoulder abduction ROM improvement over time. In the fifth session, Bruce had reduced the difference in shoulder ROM between limbs, reduced the movement compensation of leaning his torso to one side, and the pain had almost subsided. Since Bruce was self-managing his shoulder injury and resumed many normal tasks, the physiotherapist advised to Bruce that he was progressing well but still required further assessments to reduce the risk of re-injury. Bruce was given a longer-term home exercise program and encouraged to improve the strength and flexibility of his shoulder muscles.
The physiotherapist provided the WorkCover case manager with a comprehensive report detailing Bruce’s progression. Together, they developed a suitable duties plan that specified Bruce should engage in minimal overhead lifting tasks for the next 4 weeks. Despite returning to work, Bruce continued to visit his physiotherapist citing that he was motivated by directly observing improvement in his shoulder strength and ROM. After 4 weeks of limited duties work, Bruce returned to full work duties and regularly returns to the physiotherapist to ensure his movement remains on track.

Advantages of using HumanTrak
Engaging Bruce in his own care with HumanTrak empowered him to complete the prescribed rehabilitation on time. By providing Bruce with objective measures of his baseline shoulder ROM, targeted goals were set, and improvements clearly tracked over time.
When Bruce completed shoulder ROM tests, he sometimes completed the exercise with variations to avoid aggravating his pain, such as leaning his torso to the side instead of raising his arm. With video or the clinician’s eyes alone, these movement compensations would have been hard to spot. With the use of HumanTrak data, the physiotherapist clearly demonstrated client progression with objective evidence.
The WorkCover case manager was able to inform return to work decisions with objective evidence of rehabilitation improvement. By using HumanTrak as part of the rehabilitation journey, the physiotherapist was able to motivate Bruce to return beyond the standard rehabilitation time.
Monitoring progress with PROMs:
Many of the symptoms that bother clients with shoulder injuries are symptoms that can only be understood by asking the client themselves…
Given Bruce injured his shoulder, it was helpful to monitor his progress using a patient-reported outcome measure (PROM). The American Shoulder and Elbow Society score for shoulders (ASES) is a validated outcome questionnaire asking patients about their shoulder function. It can be used in rotator cuff problems, bursitis, adhesive capsulitis, and traumatic conditions such as dislocation.
Rotator cuff injuries require patients to adhere to their rehabilitation program. Therefore, adding subjective measures, such as ASES to a client’s self-reported improvement and objective progress measurements, rounds out the monitoring process and can be useful in encouraging the patient to continue with their exercises.
Here is an example of the change in ASES over time following rotator cuff injury:
With work-related injuries, there is a higher risk of delayed recovery. This is particularly apparent in the presence of the psychosocial or ‘yellow’ flags. The Orebro Musculoskeletal Screening Questionnaire is a validated tool in the workplace setting. Using the short form, 10-item questionnaire, a score over 50/100 indicates there is an 85% likelihood of delayed recovery.
Completing this questionnaire early after an injury can help practitioners explore factors such as mood, sleep, and fear-avoidance beliefs that will impact a client’s recovery and confidence in continuing with exercise before the pain has fully resolved.

If you would like more information on HumanTrak, please see our HumanTrak page or contact us (see below).
Read more HumanTrak use cases and research


Hip replacement rehab with HumanTrak (Use Case)
Tips for successful implementation of new technology


Increasing client confidence with HumanTrak
Using HumanTrak to take the guess work out of performance assessments